As our planet feels the siege-effects of an elusive pandemic, we are wise to reflect on the relationship between national health and national security. It is easy to see this relationship as always positive. Emerson put it succinctly: ‘the first wealth is health’. Decrepitude is bad for all parties – it weakens populations and imposes costs on states. But does national security ever come at the expense of public health and wellness – for example, in failed states? Might massive health failures be the signature of a failed state?
Ideally, a sustained health crisis would evoke unprecedented public-regardingness by states. Yet some states conspicuously shirk this responsibility. For example, the US has used the pandemic to pursue pre-pandemic national security agendas, like blaming foreign and domestic adversaries for instigating crises and providing cover for barriers to entry or deportation of ‘others’ lacking US citizenship. It has used the pandemic to consolidate executive power, marshal the Defense Production Act for protectionist ends and smite the World Health Organization. It has made lucrative offers to foreign firms for privileged access to universally needed coronavirus vaccine research. And, along the way, it has granted generous tax breaks to pharmaceutical giants patronizing select politicians while turning a blind eye to truly exorbitant medicine prices.
The callous politicization of national health in the US and elsewhere is a tragedy of the commons in a time of crisis. Unlike doctors, states are under no obligation to ‘first do no harm’. When such state behaviors prevail, what are citizens (and yet more vulnerable non-citizens) to do? An example from the ‘outback’ of the US – the ‘Indian Country’ in the arid Southwest, where population densities are low and COVID-19 should be incidental – provides useful insights.
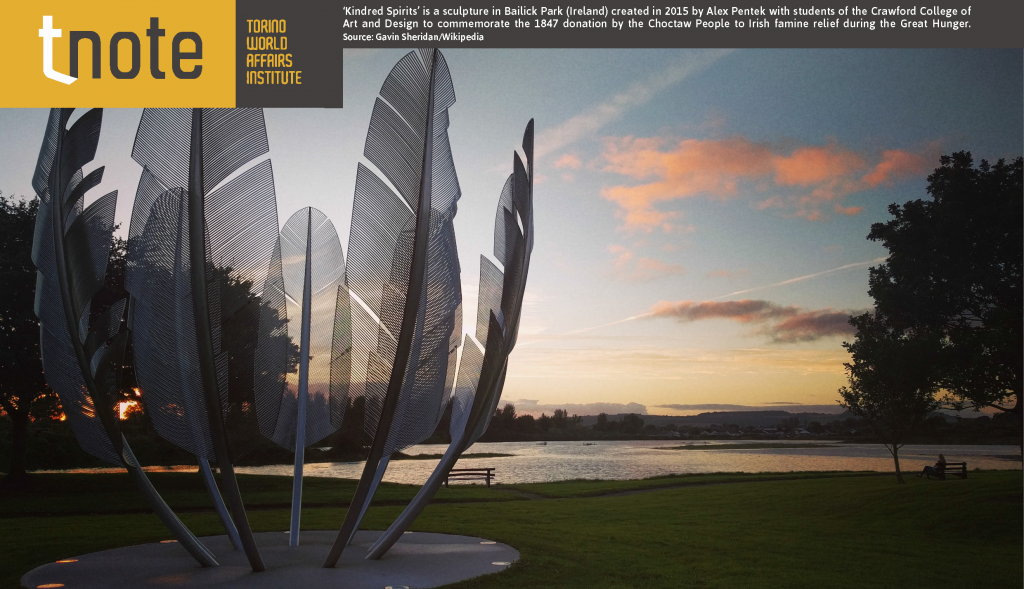
Indian nations within the US retain sovereignty thanks to treaties, ‘the supreme law of the land’ under Article 6 of the US Constitution. Their ‘national security’ relies on the fidelity of the federal government in upholding these treaty obligations. Sadly, infractions are many and show no sign of relenting during the current health crisis. The Navajo and Hopi tribes have become COVID-19 hotspots, disadvantaged by lack of water, food and medicines. In recent months, however, both tribes have found relief from an unusual source: the residents of Ireland. Via an aggressive GoFundMe campaign for food, clothing and medical relief targeting the Navajo and Hopi nations, thousands of Irish citizens have done what the US government should by law have undertaken. Many of the participating Irish donors are descended from survivors of the 1848 potato famine. They survived, in part, because of donations from Choctaw Indians who experienced a brutal removal from their own homelands in the 1830s. Whether or not ‘the Irish saved the world’, Irish Samaritans are helping to save American Indians today.

‘Kindred Spirits’ is a sculpture in Bailick Park (Ireland) created in 2015 by Alex Pentek with students of the Crawford College of Art and Design to commemorate the 1847 donation by the Choctaw People to Irish famine relief during the Great Hunger. Source: Gavin Sheridan/Wikipedia
Does this story fit with what we know from other accounts of moral turpitude by states? Among the prominent lessons of the COVID-19 crisis is that states are not even-handed in their crisis-response efforts. Some ruling elites cynically view health catastrophes as opportunities to favor their political bases, mute opposition and eliminate problems. In the past the US government famously gave smallpox-infected blankets to Indian nations, it decimated their food supplies (destroying farmlands and extinguishing millions of buffalo); even today, it discriminates against Indian farmers seeking farm loans and crop insurance. Despite well-known Navajo/Hopi contributions to national security – essential code-making and code-breaking in WWI and WWII – Native American health (and other) services are chronically under-funded. What if Irish largesse languished, and Indian public health neglect in the face of COVID-19 was laid bare?
In his insightful book The Art of Not Being Governed (2009), James Scott chronicles problematic state behaviors that challenge notions of ever-benevolent national security. States are often security havens for the few, but not the many. Bringing Scott’s insight into the present: minorities are often subject to legalized state neglect and persecution with lasting health implications – e.g., the Uyghurs in China, the Rohingya in Myanmar, the Ladinos and Gypsies in Europe, the Palestinians in Israel, the Jews on every continent and aboriginal people across the globe. The back hand of state hegemony assumes many forms: crushing taxation, conscription, forced labor, land dispossession, compulsory assimilation and an endless array of in situ displacements. These compromise access to clean water, public health, emergency care, and human rights that certainly undergird wellness.
Such breaches of the social contract are at the core of state failure. Notably, they can be present even in states vaunting their leadership in economic productivity, military strength, and material standards of living. It is precisely when states disown their populations and, as in the case of both slavery and more nuanced exploitation, predicate their wealth on intentional or de facto inequality that they ‘fail.’ State malpractice means, among other things, that the health of its population, and particularly its minority populations, is jeopardized by poor nutrition, lack of access to potable water, clean air and safe shelter, and a long list of other health and welfare indicators. Again, the US offers a well-documented example.
Surprisingly, US citizens live shorter lives with worse health than do citizens in other affluent nations, and beginning at birth. This reality affects all age groups up to age 75 and applies to multiple diseases, biological and behavioral risk factors, and injuries. Tragically, these health disadvantages are more pronounced among indigent Americans. Once again, failed states are not synonymous with weak states. According to the UN Human Development Index (HDI), the US ranks ‘very high’ (or 15th) among the 189 UN countries and territories. Its life expectancy, a component of this index, has recently grown. However, when the UN corrects this ranking for inequality, known to be severe in the US, its HDI average falls by 13.4%; this is greater than the average decrease of other ‘very high’ HDI countries when corrections for inequality are made. Little wonder that, among disenfranchised members of modern states, security often means reliance on subaltern and non-state organizations, social movements, international networks and good neighbors abroad rather than the state.
Scott is well-known for emphasizing defensive actions by those mistrustful of the state, including in times of famine and epidemic. As if commenting on the COVID-19 scourge of today, he notes that most epidemics are zoonotic diseases transferred from domesticated animals and pests that accompany them (rats, ticks, mosquitoes, fleas, mites, etc.). If zoonotic disease is expanded to include wild animals and their pests, Scott’s grasp of pandemics is highly contemporary. The same could be said for his argument that states have historically encouraged not only domestication of animals but also their crowding, concentration and intermingling with vulnerable human communities. Markets are integral to national security for most states, failed or not. Should states that deregulate the dangers and downsides of markets be viewed as neoliberal successes or as failures? In the US, where we trade off pandemic mortality for Wall Street stability (‘Death for Dow’), pathology has become an attitude as well as a disease.
How might the morbidity, mortality and inhumanity of the current pandemic expand critical thinking about national security? Numerous state responses to COVID-19 have laid bare the malaise of egregious treatment of the most vulnerable. This includes those states wearing masks of development and rarely conceived of as failing. To be affluent economically and yet impoverished in terms of health raises basic concerns about what national prosperity means and the cost at which it is achieved.
Author
Charles Geisler is a retired Professor in the Department of Development Sociology, Cornell University.
Download